About Human Kinetics

Human Kinetics, mission is to produce innovative, informative products in all areas of physical activity that help people worldwide lead healthier, more active lives.
Human Kinetics is committed to providing quality informational and educational products in the physical activity and health fields that meet the needs of our diverse customers.
---
So you or your caring partner fell and is having trouble getting back up.
Here is an edited excerpt from Health Professionals’ Guide to Physical Management of Parkinson’s Disease
found on http://www.humankinetics.com/excerpts/excerpts/assisted-floor-transfer-techniques-for-patients-with-parkinsons-disease
"Assisted floor transfer techniques for patients with Parkinson's Disease
By Miriam P. Boelen, PT"
"Assisted Floor Transfer Techniques"
When the caregiver helps the patient up from the floor, both must be kept safe. If this is not possible, additional help such as a medical alert system may be needed. If possible, the gait belt should be snug for better leverage.
Transfers should be coordinated between the patient and caregiver to ensure simultaneous maximal effort and to minimize strain on both. The caregiver can accomplish this by giving instructions such as “On the count of three try rolling onto your hands and knees” or “On the count of three try to stand up.” Because of Parkinsonian symptoms, the patient may not initiate movement at the count of three.
The caregiver should be advised of this possibility so that she or he can delay giving assistance until the patient starts. Coordination of effort will avoid placing excessive strain on the caregiver. Caregivers should be encouraged to use optimal lifting body mechanics. .....
* Assisted side lying to hands-and-knees position. The optimal hand placement of the caregiver is to position one hand under the bottom hip and the other hand under the gait belt. The caregiver pulls up on the patient’s hips as if turning a big wheel (figure 11.6, a and b). The caregiver should flex the knees to facilitate lifting with the legs rather than the back.
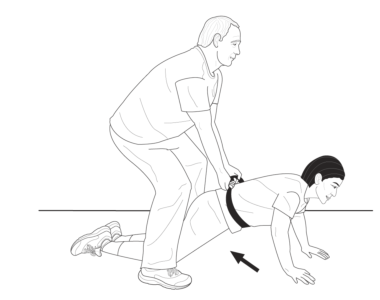
* Assisted prone to hands and knees. If the patient has strong arms, the caregiver (with proper body mechanics) can straddle the patient, grab the gait belt, and lean back while pulling up on the belt. At the same time the patient pushes with the arms (figure 11.7). As the patient walks her or his hands backward, the caregiver walks backward and guides the hips into the all-fours position.
* Assisted half kneeling to standing. The caregiver stands on the side of the patient that requires greater support. This positioning allows the patient to assist with his or her strongest side, which reduces difficulties in general. The caregiver places one hand on the gait belt and the other arm under the patient’s axilla (figure 11.8).
What to Do After a Fall
Patients often want to get up from the floor immediately after a fall. This desire may be due to the embarrassment of falling or their concern about their ability to get up. Sometimes patients do not think about the fact that after they have fallen, they cannot fall any farther and should be in no hurry to get up. Bystanders occasionally offer a helping hand, but their help may cause greater destabilization or irritate an already arthritic joint. Educating the patient about how to guide bystanders will help minimize these problems. Here are some general guidelines about what to tell your patient:
1. Do not try to get up right away.
2. Before attempting to get up, mentally note whether any areas feel injured. If you suspect injury, seek medical attention.
3. Attempt to relax for a moment before getting up.
.....
5. Before attempting to get up, someone should bring a chair close to you if needed so that you can use it for support to get up.
6. An additional chair could be placed behind you if you have difficulty turning. After you are standing, you can sit on the chair without having to turn.
This is an brief excerpt from Health Professionals’ Guide to Physical Management of Parkinson’s Disease. found on http://www.humankinetics.com/excerpts/excerpts/assisted-floor-transfer-techniques-for-patients-with-parkinsons-disease

----
A gait belt is a device used to transfer people from one position to another or from one thing to another. For example you would use a gait belt to move a patient from a standing position to a wheelchair. The gait belt is customarily made out of cotton webbing and a durable metal buckle on one end. The gait belt is worn around a patient's waist. The purpose for this is to put less strain on the back of the care giver and to provide support for the patient
--
Points to Remember: More than one caregiver may be needed. Belts with padded handles are easier to grip and increase security and control. Always transfer to resident's strongest side. Use good body mechanics and a rocking and pulling motion rather than lifting when using a belt. Belts may not be suitable for ambulation of heavy residents or residents with recent abdominal or back surgery, abdominal aneurysm, etc. Should not be used for lifting residents. Ensure belt is securely fastened and cannot be easily undone by the resident during transfer. Ensure a layer of clothing is between residents' skin and the belt to avoid abrasion. Keep resident as close as possible to caregiver during transfer. Lower bedrails, remove arms and foot rests from chairs, and other items that may obstruct the transfer



