- The Three Stages of Alzheimer's Disease
- Seven Clinical Stages of Alzhheimers
- Understanding the Dementia Experience
- Coach Broyle's Playbook for Alz Caregivers (free download or free video or you can buy hard copy)
- New York State Office for the Aging
- Aging Services Access Points, known in the elder network as ASAPs
- AOA.gov Alzheimer's resource room
- Alzheimer behaviors.pdf
- Medical is a one-stop, full service on-line medical supply
- ActiveForever Assistive Devices
- SNAP for Seniors | Senior Housing, Assisted Living, Nursing Homes
- MASS. DIVISION OF MEDICAL ASSISTANCE
- Medicare program offers limited access to two unique programs for certain beneficiaries who need a comprehensive medical and social service delivery system.
- Big Tree Murphy's - Finding the humanity
- Alzheimer's Foundation of
- America - Caring for the Nation
- Aricept's resources. Learn About Alzheimer's Disease
- The Alzheimers Store
- Alzheimer Caregiver discussions
- MASS-ALFA - Massachusetts Assisted Living Facilities
- The Medical Supply Depot.com
- SenionClix org Library
- Salmon Family of Services
- Heritage ALF Framingham
- Common Problems in early alzheimer's disease
- RUNmyERRAND: Post your errands and get help.
- National Care Planning Council
- The AGS Foundation for Health in Aging
- California Resource Centers org
- Caregiver.com; Resources - Local Massachusetts
- MedicAlert + Safe Return
- White Refrigerator Lock
- Southern California Caregiver Resource Center
- Alzherimer and Dementia Podcast Interview
- Well Spouse Association
- Alzheimer's Reading Room: Exercise for Cognition
- FCA: Family Caregiver Alliance Home
- medicaide rules
- ALZ MASS listing Support Groups for People with Alzheimers
- Thoughts from the Roller Coaster
- ElderCare Discussions
- CAREgivinghelp
- nia.nih.gov Alzheimer's Disease Education and Referral
- National Association of Professional Geriatric Care Managers
- Google Maps gains tracking feature
- Family Caregiving 101
- medicaide planning
- the alzheimer spouse - the alzheimers vanilla forum
- Sunrise ALF of Wayland
- Rosalynn Carter Institute for Caregiving
- bigtreemurphy.com/Using Usual Things.htm
- National Clearinghouse for Long Term Care
- AT&T Remote Monitor
- Caregiving Basics » Tip Cards
- http://www.bigtreemurphy.com/speech%20Topics.htm
- Alzheimer;s Massachusetts/New Hampshire Home Page
- Mail order clothing for cargeiver's clients, NH etc.,
- Pleasantries Adult Day Services - Marlborough Mass.
- Benefits Programs for seniors - NCOA's Online
- Medicaide etc information from elder law answers
- Health Information | Medical Information from Harvard
- Aricept about, Alzheimer's Disease
- Medicare Interactive Organization
- Member of the Family network U.S. Nursing Home Information resources
- AMA - American Medical Association website
- University of Maryland School of Medicine Videos
- Eligibility for the Home Care Program
- Caring From a Distance website
- The U.S. Administration on Aging (AoA)
- NIH Senior Health website
- Caring for Your Aging Parents - AgingCare.com
- Medicare.gov - MyMedicare.gov Login
- National Center on Senior Transportation: website
- Alzheimer's ORG respite care guide pdf
- Mary Anne Alzheimer's Nursing Home Facilities
- FCA-Harford-Practical Tools-Caregivers.pdf
- Caringinfo - Caring for Someone caring connections
- Move-in Information for classic assisted living facility
- Geriatric Care Managers of New England
- Finding Financial Alzheimer Assistance
- Alzstore.com - unique products to those with Alzheimers
- The Combination Care For Alzheimer's Program
- medicalnewstoday.com Assistive Technology Helps Dementia Sufferers
- Namenda Combination Treatment Right for You?
- Medicaid Waiver Programs for Assisted Living Facilities | Gilbert Guide
- Pace Program - Summit ElderCare
- AlzOnline : Alzheimer's Caregiver Support Online
- IQ Nursing Home Ratings, Directory
- Long Term Care Link - A Comprehensive Resource
- The Family Caregivers Association National
- Source for Clothing Name Labels
- Net of Care org web site
- CarePilot website
- Caring for your parents | Caring.com
- Metrowest Alzheimers Partnerships
- GPS Locators provide a more secure life for many
- Taking Care of Parents Without Going Broke - NYTimes.com
- New programs help elderly stay in their own homes
- Geocities | Respite Care Services
- Newton at Home - Website
- Mass Gov Official Website of the Office of Health and Human Services
- MA Nursing Home Quality of Care
- Z_ElderCare on-line discussion Forum
- National Association of Professional Geriatric Care Managers
- New Century Homecare Services
- blog-In-Home_Care_and_Medical_Alert_Monitoring_Solutions
- National Clearinghouse for Long Term Care
- Aging In Place Technology Watch | Industry Trends
- Caregiving Basics » Tip Cards
- California Caregiver Resource Centers
- Caregiver Homes - Caring for Elder Parent
- Elder Care Services Guides | SandwichINK.com
- Blogs - As Our Parents Grow Older
- elderlyplace.com
- Visiting Angels
- FAQ: What If I Can't Handle Caring for Someone with-incontinence
- Jewish Family Service of MetroWest
- Kaitz & Siegel Geriatric Care Managers
- Caring for Your Aging Parents - AgingCare.com
- Natick VNNA Services & Programs
- Natick Visiting Nurse Association
- Forum For Caregivers, About Caregivers, By Caregivers
- Geriatric Care Managers of New England
- Is Home Care Right For You?
- Moving Aging Parents into Your Home Are you sure?
- Medicaid
- Springwell Watertown MA
- Elderly Info 101:How to help the elderly keep their independence
- bigtreemurphy.com/Menu Resources.htm
- Legal Issues, Wills and Estate Planning - AARP
- Elder Care ABC
- Wellesley At Home
- Sudbury Angels
- Generation B - When You're Your Mother's Keeper - NYTimes.com
- Eldercare - Twitter Search #
- 5 Ways to Decide Someone you Love Needs a Caregiver
- Aging Parents | Elder Care | Senior Care
- Long Term Care Link - A Comprehensive Resource Long Term Care
- Getting Started with DIY Universal Design and Aging in Place - Inside Elder Care
- Caring for your parents | Caring.com
- Care Levels of nursing home care
- A Place for Mom a free ALF referral service
- Senior Homecare by Vjsting Angels
- AAN Issues Guideline on When People with Alzheimer’s Disease Should Stop Driving
- RxAssist database of patient prescription assistance programs
- Alzheimer Disease patient's pain behaviors
- Drug Interaction Checker
- Caregiver Guide, booklet, Home Safety for People with Alzheimer’s Disease
- Home Safety Checklist for Alzheimers in your Home, can be printed out
- Motion Detector With Remote Alarm
- Alzheimer's and Dementia Store, activitytherapy.com
- products for Wandering; Forgetfulness; Safety, Falling & Frailty, agelessdesign.com
- safety products to deal with wandering and other , ahaf.org
- safety net source a media hub with a specific focus on how caregivers can protect their loved ones from wandering and becoming missing
- LoJack® SafetyNet™ Protect and rescue anyone afflicted with Alzheimer's
- alzheimer safety products online at AllegroMedical
- Home safety checklist, alzheimers-in-your-home.com
- Home Safety Tips To Protect Those with Alzheimer'salzheimerstreatment.com
- Wandering Patient Security Systems, alznyc.org
- Free Alzheimer's Public Safety training for police, apbweb.com
- Alzheimer's Temporary Tattoo, beaconsafetyproducts.com
- Medical Alert Systems, brickhousesecurity.com
- Kitchen Safety for Someone With Alzheimer's | Care2 Healthy, care2.com
- Products for caring for alzheimers, caregiverproducts.com
- The Alzheimer's Library Incontinence Supplies for Alzheimer\'s Patients
- Caring.com Creating Home Safety for Alzheimer's patients, caring.com
- ChildSeniorSafety Home Safety for Older Adults and People with Alzheimer's, childseniorsafety.com
- Wearable Device to Find Missing Person Fast,emfinders.com
- Alzheimer's Care Home Safety, everydayhealth.com
- Safety for Those With Alzheimer's - Full Circle of Care Caregiver
- safeguarding your home for seniors with alzheimers, newlifestyles.com
- products or gadgets necessary for home safety, nia.nih.gov
- Senior Care Products. Alzheimer's parentgiving.com
- www.rafasys.com/alzheimer's-safety-0.htmlwww.rafasys.com/alzheimer's-safety-0.html
- www.research.va.gov
- Alzheimer's Safety Products. retiredbrains.com
- Alzheimer's products, righthealth.com
- fall-proofing tips for Alzheimer's disease
- Patient Safety Products - SouthwestMedical.com
- Alzheimer's Safety Catalog, sworps.tennessee.edu
- Alzheimer's Guide Dogs, thiscaringhome.org
- TotalConnect - Wireless Nurse Call Alzheimer's
- Home Safety: Room by Room Alzheimer's Research Center, zarcrom.com
- Communicating With Impaired Elderly Persons
- Nassau County Department of Senior Citizen Affairs
- Hearing Health and Alzheimer 's Disease | November 2001 | The Hearing ...
- Understanding Hearing Loss For Seniors
- Consumer Resource Directory - Community Services & Resources
- Treating Hearing Loss Important for Alzheimer 's and Dimentia
- How a Hearing Impaired Phone Can Help Grandma
- Talking To The Sight Or Hearing Impaired
- Seniors -- Alzheimer 's Disease
- Senior Health Report: Health News for Seniors About Alzheimers
- Dementia
- Senior Health Advisor 2003.1: Resource List: Alzheimer 's Disease
- VNA Care Network & Hospice's Referral Center services and insurance coverage
- Deaf/ Hearing Impaired Services
- Alzheimer 's Disease
- Triangle J Area Agency on Aging
- SENIOR SOURCE
- SeniorsSuperStores-Kitchen appliances, adaptive gadgets / tools ...
- Device that produces tiny skull vibrations a big help for hearing ...
- Although most communication changes with your loved one are due to the way Alzheimer's affects the brain, hearing problems might make communication even more difficult. Here are some tips for communicating with your loved one if he or she has a hearing problem as well as Alzheimer's disease:
- HEARING TESTS, WOMEN AND ALZHEIMER'S
- Alzheimer’s, Hearing Problems May Mimic Each Other
- Wireless TV Amplifier from Clarity Helps Hearing Impaired Folks Enjoy Television Again Recent Study Showed That 75% of People Who Experience a Hearing Loss Find It Difficult to Enjoy Television
- Alzheimer's Made Worse By Uncorrected Hearing Loss: The Inside Story
- A very useful device for the hearing impaired and helps those with minor hearing loss to avoid having to set the phone volume so loud.
- hearing and visually impaired products, our products can be used by caregivers to assist in caring for individuals with Alzheimers.
- Family Caregivers Communication Class — Part 4: Talking with Hearing Impaired Aging Parents
- How to Help a Senior Who Is Hearing Impaired. One of the hardest things to accomplish in helping a ... is the nation's second most common neurodegenerative disorder behind Alzheimer
- Attention Control Systems, Inc. Hand-held computer-based device for people with brain injury, alzheimer's disease, A.D.D. and other cognitive disorders; in Mountain View, California.
- Microsonic, Inc. Manufacturer of ear molds for hearing aids. Products are sold to hospitals and clinics.
- Alzheimers Clocks specially designed for easy viewing, day and date. .
- There may be a way to ease the symptoms of dementia and Alzheimer’s, which affect millions of people. It might be as easy as having the patient's hearing tested.
- Treating Hearing Loss Important for Alzheimer’s and Dementia
- Remember Me? A Guide to Alzheimer’s Disease and Hearing Loss
- Undiagnosed Pre-Existing Hearing Loss in Alzheimers Disease Patients?
- Hearing aids: How to choose the right one
- Hearing Aids - Products to assist individuals with impaired hearing or anyone who needs extra help hearing in this noisy world. At Independent Living Source carries a wide variety of products for anyone who may benefit from the latest technology in amplified phones from corded to cordless to vibrating alarm clocks and bed shakers
- National Program Launched to Help Low-Income Get Hearing Aids
Wednesday, September 8, 2010
Caregivers Resources
Guardian vs. Conservator: What’s the Difference? - Robert J. Kulas, P.A.
Guardian vs. Conservator: What’s the Difference? - Robert J. Kulas, P.A.
Quoted for your discussion from web site of Robert J. Kulas, Attorney, East Lake Professional Center, 2100 SE Hillmoor Drive, Suite 105, Port St. Lucie, FL 34952, Phone: (772) 398-0720
information@kulaslaw.com
--
Guardian vs. Conservator: What’s the Difference?
Sep 8, 2010
When it comes to estate planning, the terms “guardian” and “conservator” tend to come up often. There’s sometimes confusion about what a guardian does as opposed to what a conservator does. The two roles are similar but distinct.
A guardian is a court-appointed fiduciary who is responsible for ensuring that the personal, day-to-day needs of a child or incapacitated adult are taken care of. The person whose well-being the guardian is responsible for is called a “ward”. In the case of a child, often the guardian is the primary caregiver, living with the child and fulfilling a parental role. This is not always the case with an incapacitated adult. The guardian of an incapacitated adult is usually in charge of making sure that the ward gets adequate medical treatment and that the ward’s caregivers are doing an adequate job of meeting his or her personal needs.
A conservator, or guardian of the property, on the other hand, is a court-appointed fiduciary who is responsible for managing the financial affairs of a child or an incapacitated adult. The conservator takes care of real estate, manages bank accounts, and handles investments. His or her duties can range from paying bills to buying and selling stocks and bonds to managing rental property on behalf of the ward.
The main benefit of having a guardian or conservator is that the fiduciary is subject to court oversight in fulfilling his or her duties. The disadvantages to this arrangement include that, because of court involvement, guardianship or conservatorship can be an expensive and time-consuming process, and that it is a public process.
Quoted for your discussion from web site of Robert J. Kulas, Attorney, East Lake Professional Center, 2100 SE Hillmoor Drive, Suite 105, Port St. Lucie, FL 34952, Phone: (772) 398-0720
information@kulaslaw.com
--
Guardian vs. Conservator: What’s the Difference?
Sep 8, 2010
When it comes to estate planning, the terms “guardian” and “conservator” tend to come up often. There’s sometimes confusion about what a guardian does as opposed to what a conservator does. The two roles are similar but distinct.
A guardian is a court-appointed fiduciary who is responsible for ensuring that the personal, day-to-day needs of a child or incapacitated adult are taken care of. The person whose well-being the guardian is responsible for is called a “ward”. In the case of a child, often the guardian is the primary caregiver, living with the child and fulfilling a parental role. This is not always the case with an incapacitated adult. The guardian of an incapacitated adult is usually in charge of making sure that the ward gets adequate medical treatment and that the ward’s caregivers are doing an adequate job of meeting his or her personal needs.
A conservator, or guardian of the property, on the other hand, is a court-appointed fiduciary who is responsible for managing the financial affairs of a child or an incapacitated adult. The conservator takes care of real estate, manages bank accounts, and handles investments. His or her duties can range from paying bills to buying and selling stocks and bonds to managing rental property on behalf of the ward.
The main benefit of having a guardian or conservator is that the fiduciary is subject to court oversight in fulfilling his or her duties. The disadvantages to this arrangement include that, because of court involvement, guardianship or conservatorship can be an expensive and time-consuming process, and that it is a public process.
Thursday, August 19, 2010
THE Caregivers Resource Links
- The Three Stages of Alzheimer's Disease
- Seven Clinical Stages of Alzhheimers
- Understanding the Dementia Experience
- Coach Broyle's Playbook for Alz Caregivers (free download or free video or you can buy hard copy)
- New York State Office for the Aging
- Aging Services Access Points, known in the elder network as ASAPs
- AOA.gov Alzheimer's resource room
- Alzheimer behaviors.pdf
- Medical is a one-stop, full service on-line medical supply
- ActiveForever Assistive Devices
- SNAP for Seniors | Senior Housing, Assisted Living, Nursing Homes
- MASS. DIVISION OF MEDICAL ASSISTANCE
- Medicare program offers limited access to two unique programs for certain beneficiaries who need a comprehensive medical and social service delivery system.
- Big Tree Murphy's - Finding the humanity
- Alzheimer's Foundation of
- America - Caring for the Nation
- Aricept's resources. Learn About Alzheimer's Disease
- The Alzheimers Store
- Alzheimer Caregiver discussions
- MASS-ALFA - Massachusetts Assisted Living Facilities
- The Medical Supply Depot.com
- SenionClix org Library
- Salmon Family of Services
- Heritage ALF Framingham
- Common Problems in early alzheimer's disease
- RUNmyERRAND: Post your errands and get help.
- National Care Planning Council
- The AGS Foundation for Health in Aging
- California Resource Centers org
- Caregiver.com; Resources - Local Massachusetts
- MedicAlert + Safe Return
- White Refrigerator Lock
- Southern California Caregiver Resource Center
- Alzherimer and Dementia Podcast Interview
- Well Spouse Association
- Alzheimer's Reading Room: Exercise for Cognition
- FCA: Family Caregiver Alliance Home
- medicaide rules
- ALZ MASS listing Support Groups for People with Alzheimers
- Thoughts from the Roller Coaster
- ElderCare Discussions
- CAREgivinghelp
- nia.nih.gov Alzheimer's Disease Education and Referral
- National Association of Professional Geriatric Care Managers
- Google Maps gains tracking feature
- Family Caregiving 101
- medicaide planning
- the alzheimer spouse - the alzheimers vanilla forum
- Sunrise ALF of Wayland
- Rosalynn Carter Institute for Caregiving
- bigtreemurphy.com/Using Usual Things.htm
- National Clearinghouse for Long Term Care
- AT&T Remote Monitor
- Caregiving Basics » Tip Cards
- http://www.bigtreemurphy.com/speech%20Topics.htm
- Alzheimer;s Massachusetts/New Hampshire Home Page
- Mail order clothing for cargeiver's clients, NH etc.,
- Pleasantries Adult Day Services - Marlborough Mass.
- Benefits Programs for seniors - NCOA's Online
- Medicaide etc information from elder law answers
- Health Information | Medical Information from Harvard
- Aricept about, Alzheimer's Disease
- Medicare Interactive Organization
- Member of the Family network U.S. Nursing Home Information resources
- AMA - American Medical Association website
- University of Maryland School of Medicine Videos
- Eligibility for the Home Care Program
- Caring From a Distance website
- The U.S. Administration on Aging (AoA)
- NIH Senior Health website
- Caring for Your Aging Parents - AgingCare.com
- Medicare.gov - MyMedicare.gov Login
- National Center on Senior Transportation: website
- Alzheimer's ORG respite care guide pdf
- Mary Anne Alzheimer's Nursing Home Facilities
- FCA-Harford-Practical Tools-Caregivers.pdf
- Caringinfo - Caring for Someone caring connections
- Move-in Information for classic assisted living facility
- Geriatric Care Managers of New England
- Finding Financial Alzheimer Assistance
- Alzstore.com - unique products to those with Alzheimers
- The Combination Care For Alzheimer's Program
- medicalnewstoday.com Assistive Technology Helps Dementia Sufferers
- Namenda Combination Treatment Right for You?
- Medicaid Waiver Programs for Assisted Living Facilities | Gilbert Guide
- Pace Program - Summit ElderCare
- AlzOnline : Alzheimer's Caregiver Support Online
- IQ Nursing Home Ratings, Directory
- Long Term Care Link - A Comprehensive Resource
- The Family Caregivers Association National
- Source for Clothing Name Labels
- Net of Care org web site
- CarePilot website
- Caring for your parents | Caring.com
- Metrowest Alzheimers Partnerships
- GPS Locators provide a more secure life for many
- Taking Care of Parents Without Going Broke - NYTimes.com
- New programs help elderly stay in their own homes
- Geocities | Respite Care Services
- Newton at Home - Website
- Mass Gov Official Website of the Office of Health and Human Services
- MA Nursing Home Quality of Care
- Z_ElderCare on-line discussion Forum
- National Association of Professional Geriatric Care Managers
- New Century Homecare Services
- blog-In-Home_Care_and_Medical_Alert_Monitoring_Solutions
- National Clearinghouse for Long Term Care
- Aging In Place Technology Watch | Industry Trends
- Caregiving Basics » Tip Cards
- California Caregiver Resource Centers
- Caregiver Homes - Caring for Elder Parent
- Elder Care Services Guides | SandwichINK.com
- Blogs - As Our Parents Grow Older
- elderlyplace.com
- Visiting Angels
- FAQ: What If I Can't Handle Caring for Someone with-incontinence
- Jewish Family Service of MetroWest
- Kaitz & Siegel Geriatric Care Managers
- Caring for Your Aging Parents - AgingCare.com
- Natick VNNA Services & Programs
- Natick Visiting Nurse Association
- Forum For Caregivers, About Caregivers, By Caregivers
- Geriatric Care Managers of New England
- Is Home Care Right For You?
- Moving Aging Parents into Your Home Are you sure?
- Medicaid
- Springwell Watertown MA
- Elderly Info 101:How to help the elderly keep their independence
- bigtreemurphy.com/Menu Resources.htm
- Legal Issues, Wills and Estate Planning - AARP
- Elder Care ABC
- Wellesley At Home
- Sudbury Angels
- Generation B - When You're Your Mother's Keeper - NYTimes.com
- Eldercare - Twitter Search #
- 5 Ways to Decide Someone you Love Needs a Caregiver
- Aging Parents | Elder Care | Senior Care
- Long Term Care Link - A Comprehensive Resource Long Term Care
- Getting Started with DIY Universal Design and Aging in Place - Inside Elder Care
- Caring for your parents | Caring.com
- Care Levels of nursing home care
- A Place for Mom a free ALF referral service
- Senior Homecare by Vjsting Angels
- AAN Issues Guideline on When People with Alzheimer’s Disease Should Stop Driving
- RxAssist database of patient prescription assistance programs
- Alzheimer Disease patient's pain behaviors
- Drug Interaction Checker
- Caregiver Guide, booklet, Home Safety for People with Alzheimer’s Disease
- Home Safety Checklist for Alzheimers in your Home, can be printed out
- Motion Detector With Remote Alarm
- Alzheimer's and Dementia Store, activitytherapy.com
- products for Wandering; Forgetfulness; Safety, Falling & Frailty, agelessdesign.com
- safety products to deal with wandering and other , ahaf.org
- safety net source a media hub with a specific focus on how caregivers can protect their loved ones from wandering and becoming missing
- LoJack® SafetyNet™ Protect and rescue anyone afflicted with Alzheimer's
- alzheimer safety products online at AllegroMedical
- Home safety checklist, alzheimers-in-your-home.com
- Home Safety Tips To Protect Those with Alzheimer'salzheimerstreatment.com
- Wandering Patient Security Systems, alznyc.org
- Free Alzheimer's Public Safety training for police, apbweb.com
- Alzheimer's Temporary Tattoo, beaconsafetyproducts.com
- Medical Alert Systems, brickhousesecurity.com
- Kitchen Safety for Someone With Alzheimer's | Care2 Healthy, care2.com
- Products for caring for alzheimers, caregiverproducts.com
- The Alzheimer's Library Incontinence Supplies for Alzheimer\'s Patients
- Caring.com Creating Home Safety for Alzheimer's patients, caring.com
- ChildSeniorSafety Home Safety for Older Adults and People with Alzheimer's, childseniorsafety.com
- Wearable Device to Find Missing Person Fast,emfinders.com
- Alzheimer's Care Home Safety, everydayhealth.com
- Safety for Those With Alzheimer's - Full Circle of Care Caregiver
- safeguarding your home for seniors with alzheimers, newlifestyles.com
- products or gadgets necessary for home safety, nia.nih.gov
- Senior Care Products. Alzheimer's parentgiving.com
- www.rafasys.com/alzheimer's-safety-0.htmlwww.rafasys.com/alzheimer's-safety-0.html
- www.research.va.gov
- Alzheimer's Safety Products. retiredbrains.com
- Alzheimer's products, righthealth.com
- fall-proofing tips for Alzheimer's disease
- Patient Safety Products - SouthwestMedical.com
- Alzheimer's Safety Catalog, sworps.tennessee.edu
- Alzheimer's Guide Dogs, thiscaringhome.org
- TotalConnect - Wireless Nurse Call Alzheimer's
- Home Safety: Room by Room Alzheimer's Research Center, zarcrom.com
- Communicating With Impaired Elderly Persons
- Nassau County Department of Senior Citizen Affairs
- Hearing Health and Alzheimer 's Disease | November 2001 | The Hearing ...
- Understanding Hearing Loss For Seniors
- Consumer Resource Directory - Community Services & Resources
- Treating Hearing Loss Important for Alzheimer 's and Dimentia
- How a Hearing Impaired Phone Can Help Grandma
- Talking To The Sight Or Hearing Impaired
- Seniors -- Alzheimer 's Disease
- Senior Health Report: Health News for Seniors About Alzheimers
- Dementia
- Senior Health Advisor 2003.1: Resource List: Alzheimer 's Disease
- VNA Care Network & Hospice's Referral Center services and insurance coverage
- Deaf/ Hearing Impaired Services
- Alzheimer 's Disease
- Triangle J Area Agency on Aging
- SENIOR SOURCE
- SeniorsSuperStores-Kitchen appliances, adaptive gadgets / tools ...
- Device that produces tiny skull vibrations a big help for hearing ...
- Although most communication changes with your loved one are due to the way Alzheimer's affects the brain, hearing problems might make communication even more difficult. Here are some tips for communicating with your loved one if he or she has a hearing problem as well as Alzheimer's disease:
- HEARING TESTS, WOMEN AND ALZHEIMER'S
- Alzheimer’s, Hearing Problems May Mimic Each Other
- Wireless TV Amplifier from Clarity Helps Hearing Impaired Folks Enjoy Television Again Recent Study Showed That 75% of People Who Experience a Hearing Loss Find It Difficult to Enjoy Television
- Alzheimer's Made Worse By Uncorrected Hearing Loss: The Inside Story
- A very useful device for the hearing impaired and helps those with minor hearing loss to avoid having to set the phone volume so loud.
- hearing and visually impaired products, our products can be used by caregivers to assist in caring for individuals with Alzheimers.
- Family Caregivers Communication Class — Part 4: Talking with Hearing Impaired Aging Parents
- How to Help a Senior Who Is Hearing Impaired. One of the hardest things to accomplish in helping a ... is the nation's second most common neurodegenerative disorder behind Alzheimer
- Attention Control Systems, Inc. Hand-held computer-based device for people with brain injury, alzheimer's disease, A.D.D. and other cognitive disorders; in Mountain View, California.
- Microsonic, Inc. Manufacturer of ear molds for hearing aids. Products are sold to hospitals and clinics.
- Alzheimers Clocks specially designed for easy viewing, day and date. .
- There may be a way to ease the symptoms of dementia and Alzheimer’s, which affect millions of people. It might be as easy as having the patient's hearing tested.
- Treating Hearing Loss Important for Alzheimer’s and Dementia
- Remember Me? A Guide to Alzheimer’s Disease and Hearing Loss
- Undiagnosed Pre-Existing Hearing Loss in Alzheimers Disease Patients?
- Hearing aids: How to choose the right one
- Hearing Aids - Products to assist individuals with impaired hearing or anyone who needs extra help hearing in this noisy world. At Independent Living Source carries a wide variety of products for anyone who may benefit from the latest technology in amplified phones from corded to cordless to vibrating alarm clocks and bed shakers
- National Program Launched to Help Low-Income Get Hearing Aids
- Odor Eliminator & Sanitizer
Wednesday, August 18, 2010
Non-Emergency Government 311 Phone Services
311 Telephone Services

Non-Emergency Government 311 Service has been approved by the US Government as a 3-digit dedicated phone number to reach important government services from any location and at any time.
Simply dial 311 from any telephone and you will reach various non-emergency services thru out the nation.
311 is a simple, easy-to-remember telephone number which connects citizens with specially-trained city customer service representatives. They are ready to help you with your City service requests
Since 311 is a relatively new service not all localities offer 311 service at this time, especially lesser populated areas. However, its use is rapidly gaining momentum as more and more local agencies are offering it.
Things To Look for in a Retirement Home
5 Things to Look for in a Retirement Home
good article on www.smartmoney.com
"Continuing care retirement communities are probably the best prepared to deal with healthcare issues that arise as one gets further on in their golden years. This type of community hosts independent living quarters, assisted living facilities and nursing homes. That way, if a resident's health deteriorates, he or she could get the proper treatment without changing facilities. 'There will come a day when [a patient] will need [in-house, health] services,' says Holohan. 'You don't want...to change homes three or four times.'"
good article on www.smartmoney.com
"Continuing care retirement communities are probably the best prepared to deal with healthcare issues that arise as one gets further on in their golden years. This type of community hosts independent living quarters, assisted living facilities and nursing homes. That way, if a resident's health deteriorates, he or she could get the proper treatment without changing facilities. 'There will come a day when [a patient] will need [in-house, health] services,' says Holohan. 'You don't want...to change homes three or four times.'"
Thursday, August 5, 2010
What's new on BarbaraMcVicker.com? | Blog
http://nxy.in/kk7v1

As you can see, they've gone through a pretty major transition here! In case you're wondering where all the changes are, here is a brief summary:
Blog: As you can see here, Barbara now has a blog where she'll be posting great advice and eldercare news!
Expanded Resources: More online resources and recommended books!
Media & Press: A thorough compiling of all of Barbara's articles, TV appearances, and more!
Online Documents: If you're hosting Barbara for an event, or you'd just like to learn more about her, we now have an online press room and collection of event documents.
Tuesday, August 3, 2010
Paying for the ‘Institutionalized Spouse’ By CRAIG REAVES
Paying for the ‘Institutionalized Spouse’ - The New Old Age Blog - NYTimes.com

Paying for the ‘Institutionalized Spouse’
By CRAIG REAVES
Craig Reaves.Craig Reaves.
Craig Reaves, past president of the National Academy of Elder Law Attorneys, practices in Kansas City, Mo., and on occasion fields questions from New Old Age readers. You may submit your question to newoldage@nytimes.com. Please limit your inquiries to general legal issues; Mr. Reaves can’t offer personal legal advice.
Q.
What happens when one half of a married couple is retired and in need of expensive nursing home care while a younger spouse is still working and earning income? Are there options for protecting any of the income or accumulated wealth (such as retirement accounts) of the younger spouse? Or does it all have to go to pay for the care of the one who’s ill?
Saturday, July 31, 2010
Massachusetts, Elder home care programs have been cut
MetroWest feels pinch of local aid cuts - Framingham, MA - The MetroWest Daily News

Elder home care programs have been cut by $21.7 million over the last three fiscal years, a 14 percent cut when adjusted for inflation that results in approximately 2,500 fewer frail elders receiving community-based long-term care services that allow them to stay in their homes. There are now more than 2,700 elders each month on a waiting list for home care, the policy center report says.
Copyright 2010 The MetroWest Daily News. Some rights reserved
Monday, July 5, 2010
Lotsa Helping Hands A service of Alzheimer's Association
Lotsa Helping Hands - Coordination Service

Lotsa Helping Hands is a private, web-based caregiving coordination service that allows family, friends, neighbors and colleagues to create a community and assist with the daily tasks that become a challenge when caring for an aging loved one or during long-term caregiving.
Alzheimer's Association Each community includes an intuitive group calendar for scheduling tasks such as coverage or transportation to medical appointments, a platform for securely sharing vital medical, financial, and legal information with designated family members, and customizable sections for posting photos, well wishes, blogs, journals, and messages.
Now, when someone asks “what can I do to help?” the answer is “give me your name and email address” – the system takes over and allows people to sign up and start helping.
Saturday, June 26, 2010
Fell On Floor and Can't Get Up, how to help
About Human Kinetics

Human Kinetics, mission is to produce innovative, informative products in all areas of physical activity that help people worldwide lead healthier, more active lives.
Human Kinetics is committed to providing quality informational and educational products in the physical activity and health fields that meet the needs of our diverse customers.
---
So you or your caring partner fell and is having trouble getting back up.
Here is an edited excerpt from Health Professionals’ Guide to Physical Management of Parkinson’s Disease
found on http://www.humankinetics.com/excerpts/excerpts/assisted-floor-transfer-techniques-for-patients-with-parkinsons-disease
"Assisted floor transfer techniques for patients with Parkinson's Disease
By Miriam P. Boelen, PT"
"Assisted Floor Transfer Techniques"
When the caregiver helps the patient up from the floor, both must be kept safe. If this is not possible, additional help such as a medical alert system may be needed. If possible, the gait belt should be snug for better leverage.
Transfers should be coordinated between the patient and caregiver to ensure simultaneous maximal effort and to minimize strain on both. The caregiver can accomplish this by giving instructions such as “On the count of three try rolling onto your hands and knees” or “On the count of three try to stand up.” Because of Parkinsonian symptoms, the patient may not initiate movement at the count of three.
The caregiver should be advised of this possibility so that she or he can delay giving assistance until the patient starts. Coordination of effort will avoid placing excessive strain on the caregiver. Caregivers should be encouraged to use optimal lifting body mechanics. .....
* Assisted side lying to hands-and-knees position. The optimal hand placement of the caregiver is to position one hand under the bottom hip and the other hand under the gait belt. The caregiver pulls up on the patient’s hips as if turning a big wheel (figure 11.6, a and b). The caregiver should flex the knees to facilitate lifting with the legs rather than the back.
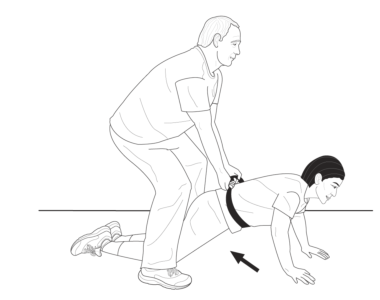
* Assisted prone to hands and knees. If the patient has strong arms, the caregiver (with proper body mechanics) can straddle the patient, grab the gait belt, and lean back while pulling up on the belt. At the same time the patient pushes with the arms (figure 11.7). As the patient walks her or his hands backward, the caregiver walks backward and guides the hips into the all-fours position.
* Assisted half kneeling to standing. The caregiver stands on the side of the patient that requires greater support. This positioning allows the patient to assist with his or her strongest side, which reduces difficulties in general. The caregiver places one hand on the gait belt and the other arm under the patient’s axilla (figure 11.8).
What to Do After a Fall
Patients often want to get up from the floor immediately after a fall. This desire may be due to the embarrassment of falling or their concern about their ability to get up. Sometimes patients do not think about the fact that after they have fallen, they cannot fall any farther and should be in no hurry to get up. Bystanders occasionally offer a helping hand, but their help may cause greater destabilization or irritate an already arthritic joint. Educating the patient about how to guide bystanders will help minimize these problems. Here are some general guidelines about what to tell your patient:
1. Do not try to get up right away.
2. Before attempting to get up, mentally note whether any areas feel injured. If you suspect injury, seek medical attention.
3. Attempt to relax for a moment before getting up.
.....
5. Before attempting to get up, someone should bring a chair close to you if needed so that you can use it for support to get up.
6. An additional chair could be placed behind you if you have difficulty turning. After you are standing, you can sit on the chair without having to turn.
This is an brief excerpt from Health Professionals’ Guide to Physical Management of Parkinson’s Disease. found on http://www.humankinetics.com/excerpts/excerpts/assisted-floor-transfer-techniques-for-patients-with-parkinsons-disease

----
A gait belt is a device used to transfer people from one position to another or from one thing to another. For example you would use a gait belt to move a patient from a standing position to a wheelchair. The gait belt is customarily made out of cotton webbing and a durable metal buckle on one end. The gait belt is worn around a patient's waist. The purpose for this is to put less strain on the back of the care giver and to provide support for the patient
--
Points to Remember: More than one caregiver may be needed. Belts with padded handles are easier to grip and increase security and control. Always transfer to resident's strongest side. Use good body mechanics and a rocking and pulling motion rather than lifting when using a belt. Belts may not be suitable for ambulation of heavy residents or residents with recent abdominal or back surgery, abdominal aneurysm, etc. Should not be used for lifting residents. Ensure belt is securely fastened and cannot be easily undone by the resident during transfer. Ensure a layer of clothing is between residents' skin and the belt to avoid abrasion. Keep resident as close as possible to caregiver during transfer. Lower bedrails, remove arms and foot rests from chairs, and other items that may obstruct the transfer
Tuesday, June 8, 2010
It takes two to tango: email version
It takes two to tango: email version - Knowledge Jolt with Jack
Putting the little elves to work.For people who watch the "personal effectiveness" discussion space, one of the favorite topics is that of dealing with email, usually with a strong focus on one person: ideas like Inbox Zero or methods for processing mail. But there is a bigger issue with email in this person is not the only player: she sends and receives emails from many others, and it is their behavior that affect her just as much as her own actions.

Putting the little elves to work.For people who watch the "personal effectiveness" discussion space, one of the favorite topics is that of dealing with email, usually with a strong focus on one person: ideas like Inbox Zero or methods for processing mail. But there is a bigger issue with email in this person is not the only player: she sends and receives emails from many others, and it is their behavior that affect her just as much as her own actions.
Wednesday, June 2, 2010
The Living Will
The Living WillA Guide To Health Care Decision Making

This copyrighted material may be freely reproduced and distributed (intact with no changes) for personal use only.
Introduction
Through advances in medical technology, some patients who formerly would have died can now be kept alive by artificial means. Sometimes a patient may desire such treatment because it is a temporary measure potentially leading to the restoration of health. At other times, such treatment may be undesirable because it may only prolong the process of dying rather than restore the patient to an acceptable quality of life. In any case, each person is seen, under the law, as having the personal right to decide whether to institute, continue or terminate such treatment. As long as a patient is mentally competent, he or she can be consulted about desired treatment. When a patient has lost the capacity to communicate, however, the situation is different.
Although New York has no statute on the question, there are state and federal court decisions that have established the right of an incompetent or comatose patient to have his or her wishes respected, as long as those wishes are known. New York law requires clear and convincing evidence of what the patient would want. Of all the various acceptable forms of evidence, a health care declaration (often called a "Living Will") can be the best. It simply documents a person's wishes concerning treatment when those wishes can no longer be personally communicated. Even in New York, such a document is recognized if it is clear, specific and unequivocal.
The following guide will help you prepare such a document if you have wishes you want respected. You should realize that if you do not express your views, treatment to maintain your life, by whatever means available, will probably be provided once you are no longer able to communicate, even if family members object. Therefore, if there are conditions under which you would not want treatment, it is important that you communicate your wishes while you are able to do so. In addition, because it is important that your wishes be documented in the most effective way possible, it is recommended that you consult your attorney in regard to the preparation of a health care declaration.
Prepared by: Jack P. Freer, M.D.
Elizabeth G. Clark, Esq.
Hodgson, Russ, Andrews, Woods & Goodyear
Attorneys At Law COPYRIGHT © 1994 Jack P. Freer, M.D. & Hodgson, Russ, Andrews, Woods & Goodyear
Better Care of the Dying
ABCD-CARING - Americans for Better Care of the Dying - Main Page

Every dying person needs to be able to count on excellent care. Americans for Better Care of the Dying (ABCD) aims to improve end-of-life care
Caring Conversations Workbook, published by the Center for Practical Bioethics
About MidBio

Midwest Bioethics Center was a community-based ethics center, founded in 1984 by a physician, an attorney, and a philosopher. Dedicated to its mission to integrate ethical considerations into healthcare decision-making throughout communities, the Center offered workshops and educational programs for professionals and lay people alike, assisted healthcare providers throughout the country in grappling with ethical issues in clinical work, and assisted administrators in integrating ethics into the organizational structure. MBC was a membership organization for both consumers and professionals.
MBC facilitated four different ethics consortia which met to study ethical issues and prepare policy guidelines.
Wednesday, May 5, 2010
Age Strong! Live Long! May is Older Americans Month
http://www.aoa.gov/AoARoot/Index.aspx
Older Americans Month Archive

Older Americans Month Archive
May is Older Americans Month
History of Older Americans Month
When Older Americans Month was established in 1963, only 17 million living Americans had reached their 65th birthdays. About a third of older Americans lived in poverty and there were few programs to meet their needs. Interest in older Americans and their concerns was growing, however. In April of 1963, President John F. Kennedy's meeting with the National Council of Senior Citizens served as a prelude to designating May as "Senior Citizens Month."
Thanks to President Jimmy Carter's 1980 designation, what was once called Senior Citizens Month, is now called "Older Americans Month," and has become a tradition.
Historically, Older Americans Month has been a time to acknowledge the contributions of past and current older persons to our country, in particular those who defended our country. Every President since JFK has issued a formal proclamation during or before the month of May asking that the entire nation pay tribute in some way to older persons in their communities. Older Americans Month is celebrated across the country through ceremonies, events, fairs and other such activities.
Past Older Americans Month Themes
* 1978 - Older Americans and the Family
* 1984 - Health: Make it Last a Lifetime
* 1985 - Help Yourself to Independence
* 1986 - Plan on Living the Rest of Your Life
* 1992 - Community Action Begins with You: Help Older Americans Help Themselves
* 1993 - No theme selected (proclamation signed on May 25, 1993)
* 1994 - Aging: An Experience of a Lifetime
* 1995 - Aging: Generations of Experience
* 1996 - Aging: A Lifetime Opportunity
* 1997 - Caregiving: Compassion in Action
* 1998 - Living Longer, Growing Stronger in America
* 1999 - Honor the Past, Imagine the Future: Towards a Society for All Ages
* 2000 - In the New Century. . . . The Future is Aging
* 2001 - The Many Faces of Aging
* 2002 - America: "A Community for all Ages"
* 2003 - What We Do Makes A Difference.”
* 2004 - Aging Well, Living Well
* 2005 - Celebrate Long-term Living
* 2006 - Choices For Independence
* 2007 - Making Choices for a Healthier Future
* 2008 - Working Together for Strong, Healthy and Supportive Communities
* 2009 - Living Today for a Better Tomorrow
* 2010 - Age Strong! Live Long!
Tuesday, May 4, 2010
The number of unpaid family caregivers in the United States now tops 65 million
The Secret Caregivers

The Secret Caregivers
By Gail Sheehy, May & June 2010
Men care for their loved ones more often than we know. Why do they hide it? Inside their silent burdens and bittersweet rewards
The number of unpaid family caregivers in the United States now tops 65 million, involving more than three in ten households, according to "Caregiving in the U.S. 2009," a report conducted by the National Alliance for Caregiving (NAC) in collaboration with AARP, and funded by the MetLife Foundation. Despite a common stereotype that caregiving is women's work, one third of American caregivers are men, the report reveals.
Caregiving in the U.S. 2009
Caregiving in the U.S. 2009

By: National Alliance for Caregiving in Collaboration with AARP; Funded by The MetLife Foundation | December 2009
Monday, May 3, 2010
How to make a visit to the physician easier for AD patient.
Pleasantries Adult Day Services - Marlboro, Massachusetts - Alternative Alzheimer’s care
Tammy Pozerycki
Owner & Director
Writes in a Pleasantries A.D.S. newsletter:

Tammy Pozerycki
Owner & Director
Writes in a Pleasantries A.D.S. newsletter:
It is important that your loved one with Alzheimer's disease have regular visits to his or her physician. These visits should address all medical and behavioral issues which may be related to Alzheimer's disease. In order to experience a productive appointment with the physician, try the following suggestions:
* Choose a "good" time of day for the appointment time (most likely morning will be best.)
* Bring along an activity that your loved one enjoys (books, sorting activity, coloring, etc) as well as a snack and water. This will prepare you for an unexpected wait time.
* Bring a list of all medication including over-the-counter. Create a list of questions in preparation of the minimal time available with the doctor.
* Depending on your situation, it may be helpful to bring someone else with you, such as a close friend or family member.
* Discuss what you can expect for the future and advance directives.
* It is good to take notes as there will be much discussed in a short amount of time.
* Be open and honest. If you are not happy or satisfied with the physician, make he or she aware of your concerns. Switching physicians can be confusing to your loved one and possibly detrimental in the longrun. If discussed, the issues may be resolved.
Monday, April 26, 2010
Northborough MA, Four Part Educational Series on Alzheimer's Disease
Free and Open to The Community at the Northborough Senior Center119 Bearfoot Road, Northborough, MA

Presented by http://www.pleasantriesads.com/
When: Part I
Tuesday, May 4th, 2010 6:00-7:00pm
"Alzheimer's............The Basics" What is Alzheimer's Disease?
Learn the basic terminology, theory, research, and up to date information.
Part II
Tuesday, May 11th, 2010 6:00-7:00pm
"Defining the 3 D's..........Dementia, Delirium, and Depression"
Learn to distinguish the similarities and differences of dementia, delirium, and depression.
Part III
Tuesday, May 18th, 2010 6:00-7:00pm
"The Alzheimer's patient, making the most of a doctor's visit"
Learn techniques and strategies to minimize the stress of any medical visit.
Part IV
Tuesday, May 25th, 2010 6:00-7:00pm
"Alternatives to Dementia Care"
Learn opportunities that can make a better day for you and your loved one with Alzheimer's disease.
To Reserve Your Space, please call: 508-393-5035
Sunday, April 25, 2010
“if you want to die, get better and die at home.”
A Graying Population, a Graying Work Force - NYTimes.com

In an aging population, the elderly are increasingly being taken care of by the elderly. Professional caregivers — almost all of them women — are one of the fastest-growing segments of the American work force, and also one of the grayest.
A recent study by PHI National, a nonprofit organization that advocates on behalf of caregivers, found that in 2008, 28 percent of home care aides were over age 55, compared with 18 percent of women in the overall work force.
The organization projects that from 2008 to 2018, the number of direct care workers, which includes those in nursing homes, will grow to 4.3 million from 3.2 million.
Wednesday, April 14, 2010

Saturday, April 3, 2010

Caregiver Assitive Technologies {Purdue edu}
Rural Caregivers - Assistive Technology

For caregivers, assistive technology, especially aids for daily living (ADLs), can make a world of difference in the lives of the individuals they care for. Whether it is modified utensils, dressing and grooming aids, or mobility aids, these devices give a person more independence to do tasks they otherwise would not be able to do with out assistance. For caregivers, assistive technology can make the job of caring for a loved one much easier.
There are many places for caregivers to turn for assistance. There are many companies that sell difference assistive devices as well as many professionals who are available to offer advice, share their knowledge and offer technical assistance.
Caregiver Resources http://cobweb.ecn.purdue.edu/~bng/BNG/Caregiving/assistivetech.html
Changing the perception and experience of aging
secondwinddreams

Second Wind Dreams® was formed in 1997, growing out of the work of geriatric specialist P.K. Beville, M.S. who co-authored Second Wind, a novel about people living in a nursing home. Over the last twelve years, SWD has become involved in more than 290 eldercare communities in 40 states, Canada and India. The mission of Second Wind Dreams® (SWD) is simple: through the fulfillment of dreams and the offering of innovative educational opportunities to caregivers and communities, SWD seeks to change the perception and experience of aging, empowering elders to age with dignity, hope and joy.
Second Wind Dreams focuses on those living in eldercare communities or in hospice care. These are our seniors who need our assistance most. Family support may be non-existent, money can be at a premium, especially for our Medicaid supported seniors, and these senior adults are often our frailest— the ones who need a dream fulfilled.
Thursday, April 1, 2010
Social Work PDF Print E-mail Written by Karen Graziano, LCSW
Social Work--THE NEW SOCIAL WORKER Online--Magazine for Social Work Students and Recent Graduates--Articles, Jobs, & More - Preparing for the Future: A Career in Gerontological Social Work

It may surprise you that the elderly are you and I. As C.S. Lewis has observed, “The future is something which everyone reaches at the rate of 60 minutes an hour, whatever he does, whoever he is.” It is one of the great equalizers. According to one of the most insightful raconteurs of our time, George Carlin, “There’s no present. There’s only the immediate future and the recent past.”
Subscribe to:
Posts (Atom)